
Experiential Validation and Design Principles
Why Methodology Matters Here
Before describing what the Isness study found, examine how it was designed, because the methodological choice is what made the findings significant.
For decades, researchers studying psychedelic experiences have relied on validated questionnaires that measure the specific qualities of non-ordinary states. unity, transcendence, feelings of sacredness, ineffability, deeply felt positive mood, and paradoxicality. The most widely used of these is the Mystical Experience Questionnaire, the MEQ30, developed and validated through Johns Hopkins and used in the major psilocybin research at both Johns Hopkins and Imperial College London.
When Glowacki and colleagues chose the MEQ30 as their primary outcome measure for a VR study, they were making a deliberate methodological statement. this experience will be evaluated by the same standard used to evaluate psychedelic mystical experiences. That choice is what allows the comparison. It's not that the researchers claimed VR was equivalent to psilocybin. It's that they used the same ruler, so the measurements can stand next to each other.
The Study Design
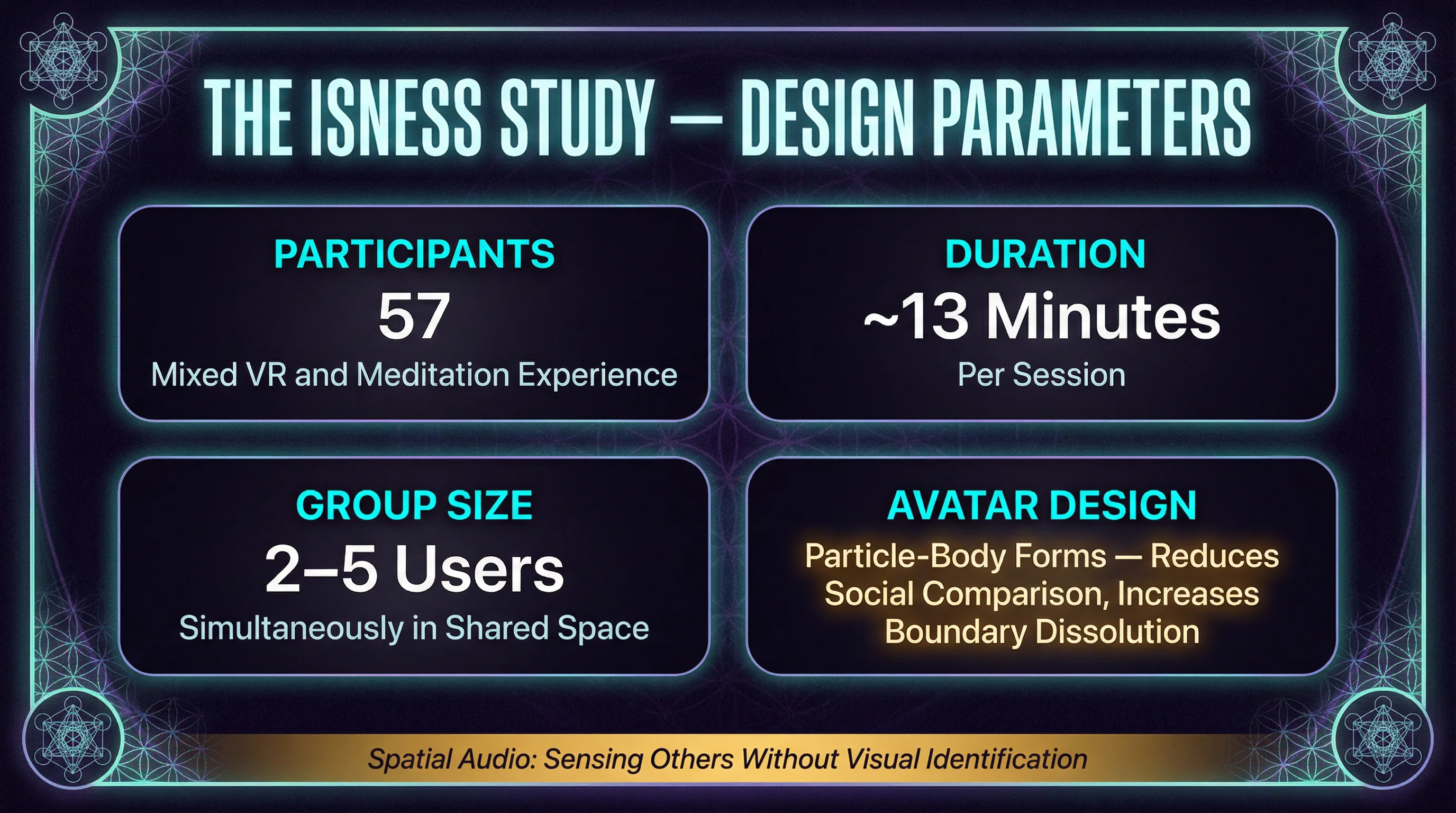
The Isness study enrolled 57 participants with varying levels of VR experience and meditation background. The VR experience lasted approximately 13 minutes. Participants entered a shared virtual environment. two to five people were present simultaneously in the same space.
The design choices were deliberate. Participants were represented as particle-body avatars rather than realistic human forms; swirling energetic shapes rather than recognizable bodies. The environment itself was abstract rather than naturalistic, geometric patterns and ambient soundscapes rather than landscapes or rooms. Movement through the space was possible, and participants could perceive each other's presence as glowing, shifting forms.
These weren't arbitrary aesthetic choices. The abstract body representation was intended to reduce social comparison and self-referential processing. The shared presence was hypothesized to amplify whatever each person was experiencing through synchronized movement and co-presence in an abstract space. The preparation before the session included intention-setting and guidance about how to enter the experience.
What the Results Showed
The average MEQ30 score across participants was above 0.6. In the MEQ30 scoring system used in Johns Hopkins psilocybin research, a score above 0.6 on the complete mystical experience subscale is the threshold for what researchers classify as a complete mystical experience. Fifty-three percent of participants met this threshold.
For context. in the Johns Hopkins high-dose psilocybin studies (30mg/70kg), approximately 61% of participants met the complete mystical experience threshold. The Isness VR participants, in a 13-minute shared VR experience with no pharmacological agent, produced scores in a comparable range.
Two additional findings stood out. First, participants who reported higher levels of presence during the experience showed higher MEQ30 scores, which is consistent with presence functioning as an amplifier for whatever the experience contains. Second, participants in multi-person sessions reported stronger mystical experience scores than comparable solo VR experiences, suggesting that shared synchronized presence in abstract virtual environments amplifies individual states.
What the Study Does and Doesn't Establish
The Isness study is landmark research, and it should be held precisely rather than loosely.
What it establishes. a 13-minute shared abstract VR experience can produce states that, measured on the same validated scale used in psilocybin research, meet the threshold for complete mystical experience in more than half of participants. That is a significant and defensible finding.
What it doesn't establish. that VR is equivalent to psilocybin as an experience, that the mechanisms are identical, that the effects have the same duration or depth, or that the finding generalizes across all VR designs. The Isness protocol was highly specific; shared multi-person design, abstract particle-body avatars, intentional preparation, a particular environment. Different designs will produce different results.
The honest summary for a practitioner. VR can produce genuine mystical experiences as measured by validated psychedelic research instruments. The conditions that produced this finding are specific and worth understanding.
Design Principles the Research Identified
Beyond the MEQ30 scores, the Isness research identified specific design principles that appear to contribute to mystical experience production in VR. These are practitioner-relevant findings, not just academic conclusions.
Abstract body representation: Energetic or particle-based avatars appear to facilitate boundary dissolution more readily than realistic human avatars, possibly because they reduce self-referential comparison and allow the sense of self to become more fluid.
Shared synchronized presence: The amplification effect of multi-person sessions suggests that co-presence in an abstract space, where participants can perceive each other without the usual social cues of realistic human interaction, creates conditions that enhance individual states.
Intentional preparation: The preparation protocol before the session, including intention-setting and guidance about how to engage with the experience, was part of the design. Stripping preparation from the protocol would likely reduce outcomes.
These aren't universal rules. They are findings from a specific study that a practitioner can use as informed starting points when designing group or individual experiences intended to facilitate deeper states.
Neural Validation and the DeepDream Findings
The DeepDream VR Research
The DeepDream VR research began from a specific hypothesis. if the visual distortions associated with psychedelic states produce measurable changes in consciousness, what happens when you produce those same visual distortions artificially?
Google's DeepDream neural network processes visual input through layers of pattern-recognition algorithms, generating outputs that resemble the visual phenomena reported during psychedelic experiences. faces, fractals, and organic forms emerging from surfaces, colors shifting and intensifying, familiar objects becoming geometrically complex. Applied to 360-degree video in real time, DeepDream VR creates a systematically hallucinogenic visual environment.
Greco and colleagues published EEG findings on DeepDream VR in 2021. The research rationale was methodologically sound. if the visual content resembles what psychedelics produce, do the neural signatures also resemble each other? The answer, with important caveats about what the resemblance does and doesn't mean, was yes in specific ways.
What the EEG Findings Showed
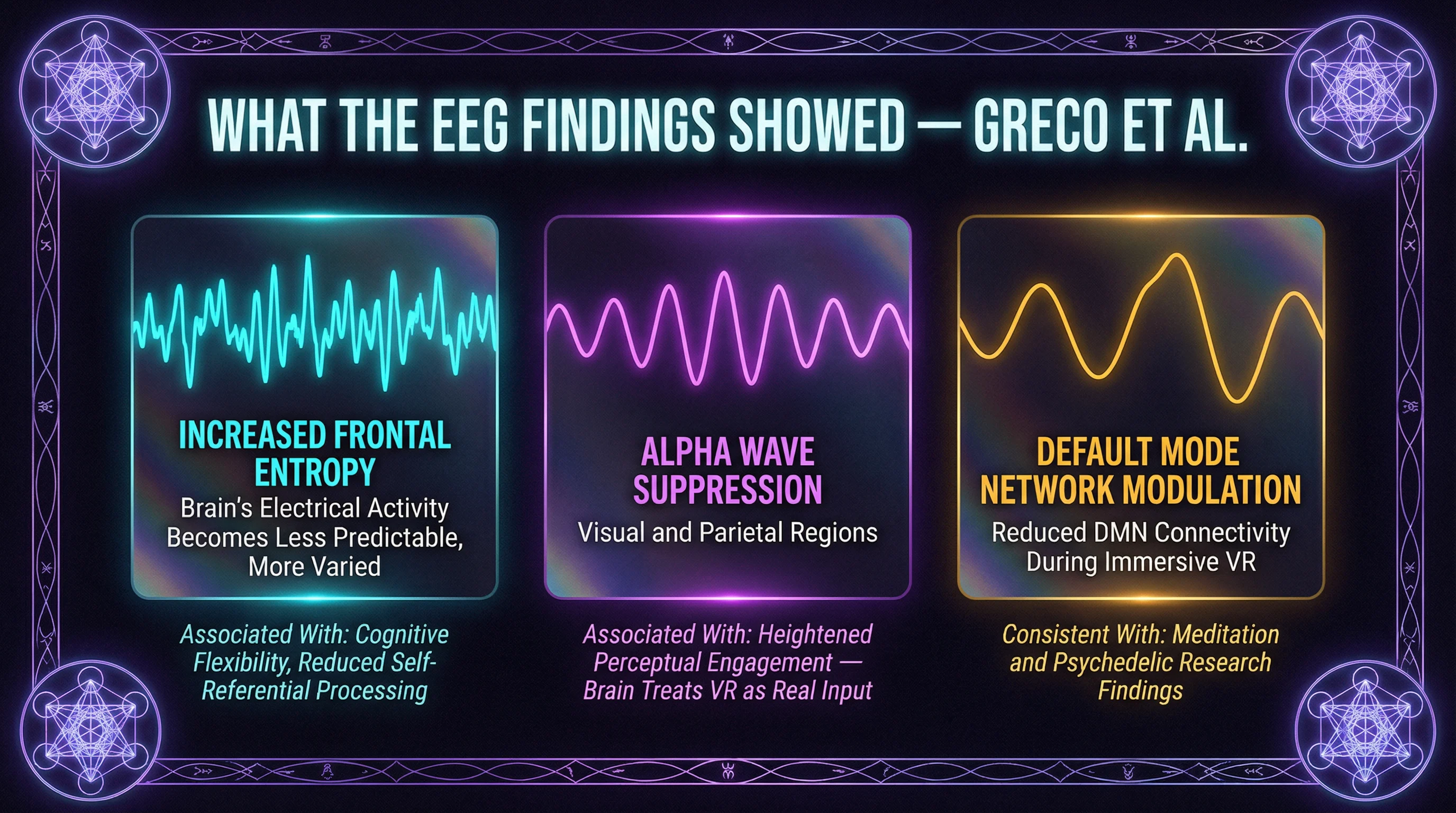
The Greco et al. findings identified three neural signatures during DeepDream VR that are of specific interest.
Increased frontal entropy: The brain's electrical activity in the frontal regions became less predictable, less repetitive, and more varied during the VR experience than at baseline. In consciousness neuroscience, frontal entropy is associated with states of increased cognitive flexibility and reduced habitual processing. Psychedelic research has found similar patterns; this is one of the proposed neural correlates of the loosening of rigid thought patterns that psychedelics and some altered states produce.
Alpha wave enhancement: Alpha waves (approximately 8-12 Hz) showed increased activity in patterns associated with meditative and relaxed but alert states. This is consistent with what EEG research shows in long-term meditators and in some psychedelic conditions.
Default Mode Network modulation: Signals consistent with reduced DMN activity were observed, echoing the finding from psychedelic and meditation research covered in Lesson 3.3.
These three signatures together describe a brain in a state that differs measurably from ordinary waking consciousness.
What These Findings Mean in Plain Terms
The three neural signatures are not just abstract measurements; they have interpretable meaning for what is happening in the person's experience.
Increased frontal entropy means the brain is processing information less predictably and more flexibly than usual. The habitual patterns that constitute ordinary self-talk, ruminative loops, and rigid cognitive frameworks require the brain to run familiar sequences reliably. When frontal entropy increases, those sequences become less stable. The person may experience this as thoughts feeling less fixed, associations becoming more fluid, or the usual mental furniture feeling less solid.
Alpha wave enhancement is associated with a state of relaxed, receptive alertness rather than either anxious arousal or passive drowsiness. It is the neural state often associated with creative thinking, open attention, and meditative calm. Subjectively this tends to feel like a quality of open, easy presence rather than directed focus or drifting inattention.
DMN modulation connects directly to what was covered in Lesson 3.3. when the Default Mode Network quiets, the sense of being a separate self narrating experience from the inside softens. The boundary between observer and observed becomes less sharp.
The Honest Calibration
These neural findings are real and deserve serious consideration. They are also early evidence, and should be communicated as such.
The Greco et al. study is a single published study rather than a replicated finding. The neural signatures it identified resemble patterns seen in psychedelic and meditative states; they are not identical to them, and the study does not claim they are. VR-induced frontal entropy and psychedelic-induced frontal entropy may reflect similar broad mechanisms or may reflect different underlying processes that produce similar-looking EEG signatures. That distinction matters and the research doesn't yet resolve it.
What the neural evidence establishes at this stage. the brain responds to VR-induced altered states as neurological events, not as imagination or performance. The EEG changes are measurable and distinct from baseline. They show patterns that overlap with, but are not identical to, patterns seen in pharmacological and meditative altered states.
When a skeptic argues that VR altered states are 'not real' because no chemical change occurs, the neural evidence is a direct and calibrated response. the brain produces measurable neurological changes in response to VR. The changes are real. Whether they are identical to psychedelic changes is a different, more complex question.
Why Neural Validation Matters for the Field
The experiential evidence, the MEQ30 scores from the Isness study, speaks to what people report about their subjective experience. Neural evidence speaks to a different level than what the brain is doing that corresponds to those reports.
Both are needed. Subjective reports without neural correlates leave the field vulnerable to the claim that what participants are measuring is expectation or suggestion. Neural changes without subjective significance would be interesting neuroscience without clear therapeutic or experiential relevance. The two evidence streams together make a stronger case than either makes alone.
For practitioners, this is the architecture of a credible answer when someone asks whether cyberdelic experiences are scientifically real. there are two independent levels of evidence. People report experiences that, measured on validated scales, meet established thresholds for significant non-ordinary states. And there are measurable neurological changes that correspond to those reports. Neither level of evidence is complete on its own. Together, they establish that something is happening that is both subjectively significant and neurologically real.
The Spectrum of Therapeutic Evidence
The Evidence Spectrum
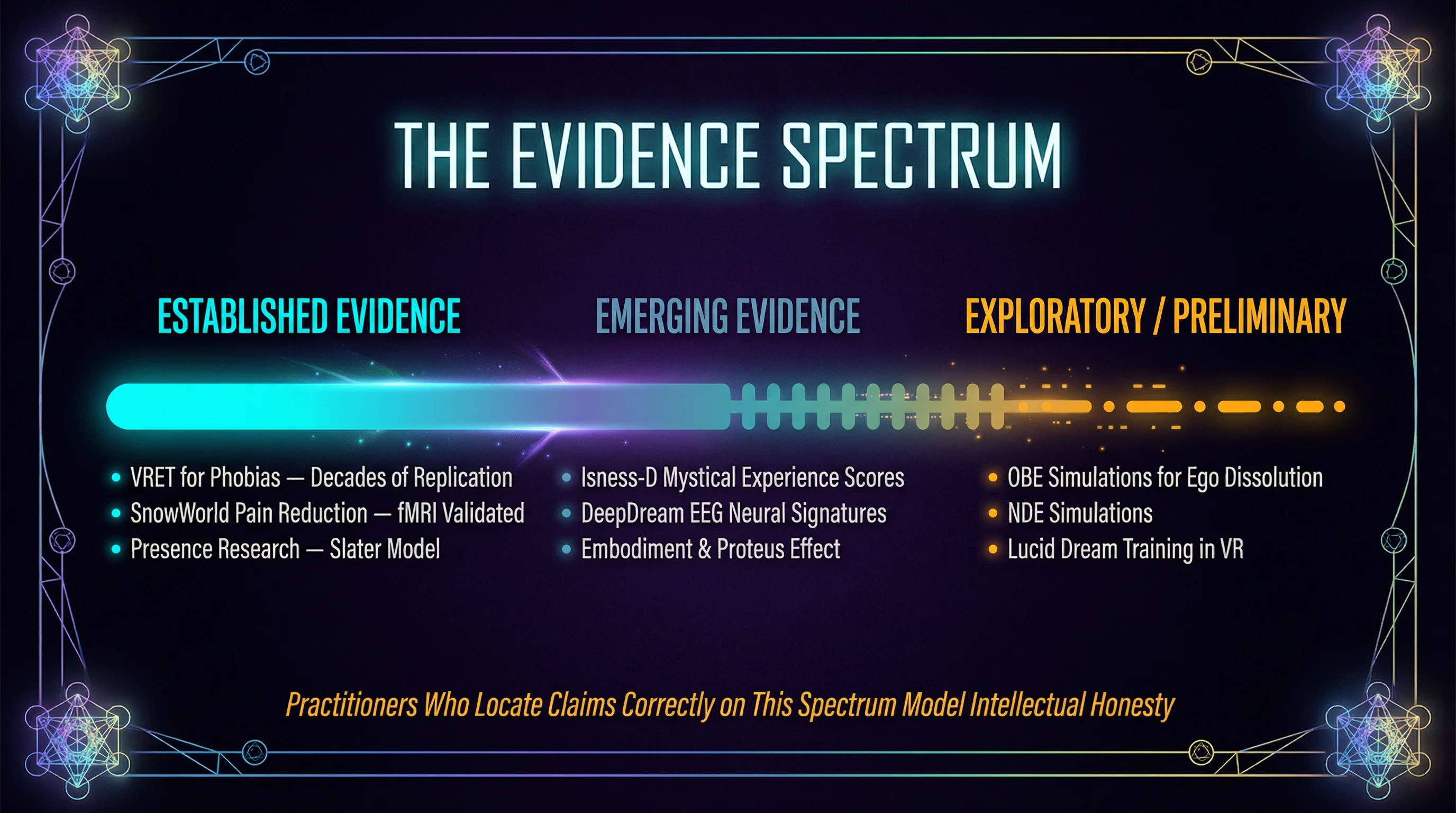
Not all claims about cyberdelic VR rest on equally solid ground. Some rest on decades of replicated clinical research. Some rest on a handful of promising studies. Some rest on plausible hypotheses with early preliminary support. Practitioners who can locate each type of claim in its correct position on this spectrum are doing something essential for the field. they are modeling the intellectual honesty that gives the work its credibility.
The three evidence streams covered in this lesson each sit at a different point on that spectrum. Here is where each one stands.
Application Area | Evidence Level | Representative Research | Clinical Status |
|---|---|---|---|
VR Exposure Therapy (phobias, anxiety) | Most Established | 20+ years of replicated studies; 80%+ effectiveness rates | Clinically validated |
Pain Management VR (SnowWorld) | Most Established | Multiple published clinical trials; 35-50% pain reduction with fMRI confirmation | Clinically validated |
Depression, PTSD, Social Anxiety VR | Developing | Multiple studies with reasonably consistent findings across research groups | Promising; not yet standard of care |
Consciousness Expansion and Mystical Experience | Early Research | Isness study (2020); significant single-study finding, not yet replicated at scale | Research phase |
The cyberdelic field, like any emerging field, is prone to overclaiming. A researcher, clinician, or potential client who encounters an overclaim and recognizes it will extend that skepticism to the legitimate evidence as well. The practitioner's job is not to be a skeptic or a promoter. It is to be accurate.
The Most Established Stream: Therapeutic VR
VR exposure therapy for anxiety disorders and phobias is the most thoroughly established application in the cyberdelic evidence base. Research in this area began in the early 1990s at USC and Yale and has accumulated across more than twenty years of replicated studies. Clinical effectiveness rates for VR exposure therapy in anxiety disorders are in the range of 80% or above, comparable to gold-standard in-vivo exposure therapy. This is not emerging evidence; it is clinically validated.
Pain management using VR is nearly as well established. Hunter Hoffman and colleagues at the University of Washington's Human Interface Technology Lab developed and studied SnowWorld, a VR environment specifically designed for burn patients undergoing painful wound debridement procedures. Multiple published studies found that VR reduced pain ratings during procedures by 35-50% compared to control conditions, with corresponding reductions in pain-related brain activity in fMRI. These findings have been replicated and have influenced clinical pain management practice in burn care and related fields.
These two applications are the foundation of the therapeutic evidence base. A practitioner citing them is citing established, replicated clinical findings.
The Middle Stream: Mental Health Applications
Beyond exposure therapy and pain management, VR applications for broader mental health purposes, including depression, PTSD, social anxiety, and trauma processing, represent a more varied evidence landscape.
Some of these applications have multiple published studies and reasonably consistent findings across research groups. VR-based cognitive behavioral therapy for social anxiety, for example, has accumulated enough evidence to support clinical use in specialized contexts. VR applications for PTSD are in active clinical trials at several research institutions, with published pilot findings that are promising but not yet at the replication level of VRET for specific phobias.
Others are earlier in the research arc. single published studies, pilot protocols, or pre-post designs without randomized controls. The findings are often clinically plausible and consistent with the mechanisms described in Lesson 3.3, but they don't yet carry the same evidential weight as the exposure therapy and pain management literature.
Practitioners working in mental health contexts need to be specific about where their particular application sits. 'VR has been clinically validated for anxiety disorders' is accurate. 'VR therapy is proven for trauma processing' is not yet accurate at the same level of certainty.
The Emerging Stream: Consciousness Expansion Applications
Cyberdelic applications specifically designed for consciousness expansion, mystical experience production, personal development, and non-clinical transformation sit at the earliest point in the research arc. The Isness study is the landmark piece of evidence here, and it is genuinely landmark. a single well-designed study with significant findings, not yet replicated at scale.
The Isness finding, that VR can produce MEQ30-measured mystical experiences in more than half of participants, is real and defensible. What it doesn't yet provide is the accumulated research foundation that exposure therapy has. multiple independent research groups, varied populations, different protocols producing consistent results.
This doesn't mean consciousness-expansion applications are less real or less valuable. It means the evidence base is younger. The honest framing for practitioners is. early research suggests that well-designed VR experiences can produce states measurable as complete mystical experiences, with design principles that appear to influence outcomes. The Isness study is a strong foundation. It is not yet a replicated clinical evidence base.
This distinction protects practitioner credibility. It also, over time, protects the field. overclaiming the consciousness-expansion evidence while the therapeutic evidence is the more robust stream conflates two very different levels of evidence into a single rhetorical gesture.
What the Honest Practitioner Answer Sounds Like
When a client, colleague, or skeptic asks whether there is evidence for cyberdelic VR, the accurate answer depends on which application is being discussed. Here is what honest calibration sounds like in practice.
For therapeutic applications.
VR exposure therapy has more than twenty years of replicated research behind it and clinical effectiveness rates comparable to gold-standard in-person therapy. Pain management VR has multiple published clinical studies showing 35-50% reduction in procedural pain. Those are established findings. Broader mental health applications are in active clinical development with promising but more varied evidence.
For consciousness expansion.
The leading evidence is a 2020 PLOS ONE study showing that a specific VR protocol produced mystical experience scores comparable to high-dose psilocybin in more than half of participants. That's a significant finding. It's also a single study, not a replicated clinical evidence base. Early neural research shows measurable brain changes during altered-state VR. Together, this is real evidence that something significant is happening; it's not yet the same depth of evidence as the therapeutic applications.
This is not underselling the field. It is communicating accurately in a way that holds across any level of scrutiny.
Experiential Validation and Design Principles
Why Methodology Matters Here
Before describing what the Isness study found, examine how it was designed, because the methodological choice is what made the findings significant.
For decades, researchers studying psychedelic experiences have relied on validated questionnaires that measure the specific qualities of non-ordinary states. unity, transcendence, feelings of sacredness, ineffability, deeply felt positive mood, and paradoxicality. The most widely used of these is the Mystical Experience Questionnaire, the MEQ30, developed and validated through Johns Hopkins and used in the major psilocybin research at both Johns Hopkins and Imperial College London.
When Glowacki and colleagues chose the MEQ30 as their primary outcome measure for a VR study, they were making a deliberate methodological statement. this experience will be evaluated by the same standard used to evaluate psychedelic mystical experiences. That choice is what allows the comparison. It's not that the researchers claimed VR was equivalent to psilocybin. It's that they used the same ruler, so the measurements can stand next to each other.
The Study Design
The Isness study enrolled 57 participants with varying levels of VR experience and meditation background. The VR experience lasted approximately 13 minutes. Participants entered a shared virtual environment. two to five people were present simultaneously in the same space.
The design choices were deliberate. Participants were represented as particle-body avatars rather than realistic human forms; swirling energetic shapes rather than recognizable bodies. The environment itself was abstract rather than naturalistic, geometric patterns and ambient soundscapes rather than landscapes or rooms. Movement through the space was possible, and participants could perceive each other's presence as glowing, shifting forms.
These weren't arbitrary aesthetic choices. The abstract body representation was intended to reduce social comparison and self-referential processing. The shared presence was hypothesized to amplify whatever each person was experiencing through synchronized movement and co-presence in an abstract space. The preparation before the session included intention-setting and guidance about how to enter the experience.
What the Results Showed
The average MEQ30 score across participants was above 0.6. In the MEQ30 scoring system used in Johns Hopkins psilocybin research, a score above 0.6 on the complete mystical experience subscale is the threshold for what researchers classify as a complete mystical experience. Fifty-three percent of participants met this threshold.
For context. in the Johns Hopkins high-dose psilocybin studies (30mg/70kg), approximately 61% of participants met the complete mystical experience threshold. The Isness VR participants, in a 13-minute shared VR experience with no pharmacological agent, produced scores in a comparable range.
Two additional findings stood out. First, participants who reported higher levels of presence during the experience showed higher MEQ30 scores, which is consistent with presence functioning as an amplifier for whatever the experience contains. Second, participants in multi-person sessions reported stronger mystical experience scores than comparable solo VR experiences, suggesting that shared synchronized presence in abstract virtual environments amplifies individual states.
What the Study Does and Doesn't Establish
The Isness study is landmark research, and it should be held precisely rather than loosely.
What it establishes. a 13-minute shared abstract VR experience can produce states that, measured on the same validated scale used in psilocybin research, meet the threshold for complete mystical experience in more than half of participants. That is a significant and defensible finding.
What it doesn't establish. that VR is equivalent to psilocybin as an experience, that the mechanisms are identical, that the effects have the same duration or depth, or that the finding generalizes across all VR designs. The Isness protocol was highly specific; shared multi-person design, abstract particle-body avatars, intentional preparation, a particular environment. Different designs will produce different results.
The honest summary for a practitioner. VR can produce genuine mystical experiences as measured by validated psychedelic research instruments. The conditions that produced this finding are specific and worth understanding.
Design Principles the Research Identified
Beyond the MEQ30 scores, the Isness research identified specific design principles that appear to contribute to mystical experience production in VR. These are practitioner-relevant findings, not just academic conclusions.
Abstract body representation: Energetic or particle-based avatars appear to facilitate boundary dissolution more readily than realistic human avatars, possibly because they reduce self-referential comparison and allow the sense of self to become more fluid.
Shared synchronized presence: The amplification effect of multi-person sessions suggests that co-presence in an abstract space, where participants can perceive each other without the usual social cues of realistic human interaction, creates conditions that enhance individual states.
Intentional preparation: The preparation protocol before the session, including intention-setting and guidance about how to engage with the experience, was part of the design. Stripping preparation from the protocol would likely reduce outcomes.
These aren't universal rules. They are findings from a specific study that a practitioner can use as informed starting points when designing group or individual experiences intended to facilitate deeper states.
Neural Validation and the DeepDream Findings
The DeepDream VR Research
The DeepDream VR research began from a specific hypothesis. if the visual distortions associated with psychedelic states produce measurable changes in consciousness, what happens when you produce those same visual distortions artificially?
Google's DeepDream neural network processes visual input through layers of pattern-recognition algorithms, generating outputs that resemble the visual phenomena reported during psychedelic experiences. faces, fractals, and organic forms emerging from surfaces, colors shifting and intensifying, familiar objects becoming geometrically complex. Applied to 360-degree video in real time, DeepDream VR creates a systematically hallucinogenic visual environment.
Greco and colleagues published EEG findings on DeepDream VR in 2021. The research rationale was methodologically sound. if the visual content resembles what psychedelics produce, do the neural signatures also resemble each other? The answer, with important caveats about what the resemblance does and doesn't mean, was yes in specific ways.
What the EEG Findings Showed
The Greco et al. findings identified three neural signatures during DeepDream VR that are of specific interest.
Increased frontal entropy: The brain's electrical activity in the frontal regions became less predictable, less repetitive, and more varied during the VR experience than at baseline. In consciousness neuroscience, frontal entropy is associated with states of increased cognitive flexibility and reduced habitual processing. Psychedelic research has found similar patterns; this is one of the proposed neural correlates of the loosening of rigid thought patterns that psychedelics and some altered states produce.
Alpha wave enhancement: Alpha waves (approximately 8-12 Hz) showed increased activity in patterns associated with meditative and relaxed but alert states. This is consistent with what EEG research shows in long-term meditators and in some psychedelic conditions.
Default Mode Network modulation: Signals consistent with reduced DMN activity were observed, echoing the finding from psychedelic and meditation research covered in Lesson 3.3.
These three signatures together describe a brain in a state that differs measurably from ordinary waking consciousness.
What These Findings Mean in Plain Terms
The three neural signatures are not just abstract measurements; they have interpretable meaning for what is happening in the person's experience.
Increased frontal entropy means the brain is processing information less predictably and more flexibly than usual. The habitual patterns that constitute ordinary self-talk, ruminative loops, and rigid cognitive frameworks require the brain to run familiar sequences reliably. When frontal entropy increases, those sequences become less stable. The person may experience this as thoughts feeling less fixed, associations becoming more fluid, or the usual mental furniture feeling less solid.
Alpha wave enhancement is associated with a state of relaxed, receptive alertness rather than either anxious arousal or passive drowsiness. It is the neural state often associated with creative thinking, open attention, and meditative calm. Subjectively this tends to feel like a quality of open, easy presence rather than directed focus or drifting inattention.
DMN modulation connects directly to what was covered in Lesson 3.3. when the Default Mode Network quiets, the sense of being a separate self narrating experience from the inside softens. The boundary between observer and observed becomes less sharp.
The Honest Calibration
These neural findings are real and deserve serious consideration. They are also early evidence, and should be communicated as such.
The Greco et al. study is a single published study rather than a replicated finding. The neural signatures it identified resemble patterns seen in psychedelic and meditative states; they are not identical to them, and the study does not claim they are. VR-induced frontal entropy and psychedelic-induced frontal entropy may reflect similar broad mechanisms or may reflect different underlying processes that produce similar-looking EEG signatures. That distinction matters and the research doesn't yet resolve it.
What the neural evidence establishes at this stage. the brain responds to VR-induced altered states as neurological events, not as imagination or performance. The EEG changes are measurable and distinct from baseline. They show patterns that overlap with, but are not identical to, patterns seen in pharmacological and meditative altered states.
When a skeptic argues that VR altered states are 'not real' because no chemical change occurs, the neural evidence is a direct and calibrated response. the brain produces measurable neurological changes in response to VR. The changes are real. Whether they are identical to psychedelic changes is a different, more complex question.
Why Neural Validation Matters for the Field
The experiential evidence, the MEQ30 scores from the Isness study, speaks to what people report about their subjective experience. Neural evidence speaks to a different level than what the brain is doing that corresponds to those reports.
Both are needed. Subjective reports without neural correlates leave the field vulnerable to the claim that what participants are measuring is expectation or suggestion. Neural changes without subjective significance would be interesting neuroscience without clear therapeutic or experiential relevance. The two evidence streams together make a stronger case than either makes alone.
For practitioners, this is the architecture of a credible answer when someone asks whether cyberdelic experiences are scientifically real. there are two independent levels of evidence. People report experiences that, measured on validated scales, meet established thresholds for significant non-ordinary states. And there are measurable neurological changes that correspond to those reports. Neither level of evidence is complete on its own. Together, they establish that something is happening that is both subjectively significant and neurologically real.
The Spectrum of Therapeutic Evidence
The Evidence Spectrum
Not all claims about cyberdelic VR rest on equally solid ground. Some rest on decades of replicated clinical research. Some rest on a handful of promising studies. Some rest on plausible hypotheses with early preliminary support. Practitioners who can locate each type of claim in its correct position on this spectrum are doing something essential for the field. they are modeling the intellectual honesty that gives the work its credibility.
The three evidence streams covered in this lesson each sit at a different point on that spectrum. Here is where each one stands.
Application Area | Evidence Level | Representative Research | Clinical Status |
|---|---|---|---|
VR Exposure Therapy (phobias, anxiety) | Most Established | 20+ years of replicated studies; 80%+ effectiveness rates | Clinically validated |
Pain Management VR (SnowWorld) | Most Established | Multiple published clinical trials; 35-50% pain reduction with fMRI confirmation | Clinically validated |
Depression, PTSD, Social Anxiety VR | Developing | Multiple studies with reasonably consistent findings across research groups | Promising; not yet standard of care |
Consciousness Expansion and Mystical Experience | Early Research | Isness study (2020); significant single-study finding, not yet replicated at scale | Research phase |
The cyberdelic field, like any emerging field, is prone to overclaiming. A researcher, clinician, or potential client who encounters an overclaim and recognizes it will extend that skepticism to the legitimate evidence as well. The practitioner's job is not to be a skeptic or a promoter. It is to be accurate.
The Most Established Stream: Therapeutic VR
VR exposure therapy for anxiety disorders and phobias is the most thoroughly established application in the cyberdelic evidence base. Research in this area began in the early 1990s at USC and Yale and has accumulated across more than twenty years of replicated studies. Clinical effectiveness rates for VR exposure therapy in anxiety disorders are in the range of 80% or above, comparable to gold-standard in-vivo exposure therapy. This is not emerging evidence; it is clinically validated.
Pain management using VR is nearly as well established. Hunter Hoffman and colleagues at the University of Washington's Human Interface Technology Lab developed and studied SnowWorld, a VR environment specifically designed for burn patients undergoing painful wound debridement procedures. Multiple published studies found that VR reduced pain ratings during procedures by 35-50% compared to control conditions, with corresponding reductions in pain-related brain activity in fMRI. These findings have been replicated and have influenced clinical pain management practice in burn care and related fields.
These two applications are the foundation of the therapeutic evidence base. A practitioner citing them is citing established, replicated clinical findings.
The Middle Stream: Mental Health Applications
Beyond exposure therapy and pain management, VR applications for broader mental health purposes, including depression, PTSD, social anxiety, and trauma processing, represent a more varied evidence landscape.
Some of these applications have multiple published studies and reasonably consistent findings across research groups. VR-based cognitive behavioral therapy for social anxiety, for example, has accumulated enough evidence to support clinical use in specialized contexts. VR applications for PTSD are in active clinical trials at several research institutions, with published pilot findings that are promising but not yet at the replication level of VRET for specific phobias.
Others are earlier in the research arc. single published studies, pilot protocols, or pre-post designs without randomized controls. The findings are often clinically plausible and consistent with the mechanisms described in Lesson 3.3, but they don't yet carry the same evidential weight as the exposure therapy and pain management literature.
Practitioners working in mental health contexts need to be specific about where their particular application sits. 'VR has been clinically validated for anxiety disorders' is accurate. 'VR therapy is proven for trauma processing' is not yet accurate at the same level of certainty.
The Emerging Stream: Consciousness Expansion Applications
Cyberdelic applications specifically designed for consciousness expansion, mystical experience production, personal development, and non-clinical transformation sit at the earliest point in the research arc. The Isness study is the landmark piece of evidence here, and it is genuinely landmark. a single well-designed study with significant findings, not yet replicated at scale.
The Isness finding, that VR can produce MEQ30-measured mystical experiences in more than half of participants, is real and defensible. What it doesn't yet provide is the accumulated research foundation that exposure therapy has. multiple independent research groups, varied populations, different protocols producing consistent results.
This doesn't mean consciousness-expansion applications are less real or less valuable. It means the evidence base is younger. The honest framing for practitioners is. early research suggests that well-designed VR experiences can produce states measurable as complete mystical experiences, with design principles that appear to influence outcomes. The Isness study is a strong foundation. It is not yet a replicated clinical evidence base.
This distinction protects practitioner credibility. It also, over time, protects the field. overclaiming the consciousness-expansion evidence while the therapeutic evidence is the more robust stream conflates two very different levels of evidence into a single rhetorical gesture.
What the Honest Practitioner Answer Sounds Like
When a client, colleague, or skeptic asks whether there is evidence for cyberdelic VR, the accurate answer depends on which application is being discussed. Here is what honest calibration sounds like in practice.
For therapeutic applications.
VR exposure therapy has more than twenty years of replicated research behind it and clinical effectiveness rates comparable to gold-standard in-person therapy. Pain management VR has multiple published clinical studies showing 35-50% reduction in procedural pain. Those are established findings. Broader mental health applications are in active clinical development with promising but more varied evidence.
For consciousness expansion.
The leading evidence is a 2020 PLOS ONE study showing that a specific VR protocol produced mystical experience scores comparable to high-dose psilocybin in more than half of participants. That's a significant finding. It's also a single study, not a replicated clinical evidence base. Early neural research shows measurable brain changes during altered-state VR. Together, this is real evidence that something significant is happening; it's not yet the same depth of evidence as the therapeutic applications.
This is not underselling the field. It is communicating accurately in a way that holds across any level of scrutiny.



Continue your path
Mark this lesson complete, then move forward.